Common gene variant creates paradoxical drug response for irregular heartbeat
Research in Jon Silva’s lab highlights call for importance of genetic testing for precision medicine
Irregular heartbeat, or arrythmia, can be treated with various procedures or medication, but not all medications work for all patients. In fact, one arrythmia medication can actually cause arrythmia in people with a common genetic variant, creating the need for personalized medicine to provide patients with the most beneficial outcome.
Jon Silva, professor of biomedical engineering in the McKelvey School of Engineering at Washington University in St. Louis, and Martina Marras, a doctoral student in his lab, made the discovery by screening four genetic variants to see if any of them altered the effectiveness of the drug mexiletine. The more than 50-year-old drug is commonly used to treat cardiac arrhythmia but only works in about 20% of patients. Their work raises a call to reconsider how drugs to treat arrhythmia are prescribed as well as how more genetic testing in patients could guide that reconsideration.
Results of their research were published online in the Journal of Precision Medicine March 18, 2026.
Silva’s lab has been studying the genetic causes of arrhythmia for more than a decade and has considered whether there were common variants that didn’t interfere with the sodium channel function to cause disease but changed how patients responded to mexiletine. The new research stems from a prior study, published in Circulation Research in 2019, that showed that rare SCN5A mutations connected to Long QT Syndrome type 3 can alter a patient’s response to mexiletine.
In the new research, they screened four common SCN5A variants — R34C, S524Y, H558R and S1103Y. They found that the S1103Y variant was one that changed response to mexiletine. S1103Y is a single-letter change in the SCN5A gene, which encodes the protein Nav1.5, a voltage-gated sodium channel central to the electrical activity of the heart and the primary target of a class of antiarrhythmic drugs that includes lidocaine and mexiletine. The variant appears in 13% of African-descendant populations.
“This is a significant precision medicine finding,” Silva said. “It shows that a genetic variant previously considered benign can dramatically alter how a patient responds to a medication, even when the variant is harmless otherwise.”
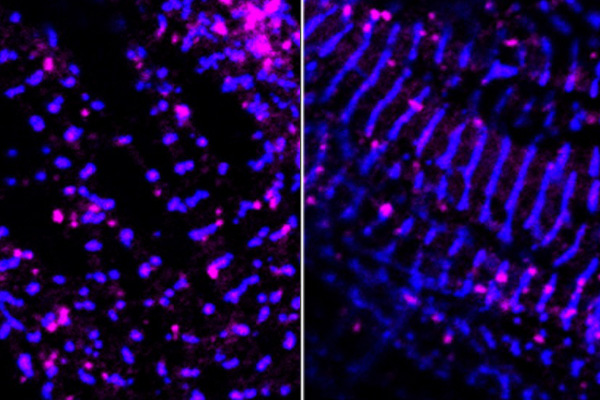
Marras and the team used induced pluripotent stem cells (iPSC) from a patient donor as well as from a genetically matched cell line to grow heart cells that grow sodium channels. In cells carrying two copies of S1103Y, mexiletine caused an increase in late sodium current, a small but persistent trickle of electrical charge that continues flowing through the sodium channel well after it should have shut off. When it increases, it delays the electrical reset that occurs after each heartbeat, prolonging the action potential in a way that is associated with dangerous arrhythmias.
“This is precisely the kind of effect that a drug like mexiletine is supposed to prevent, not cause,” Silva said.
They also found that in cells carrying only one copy of S1103Y, there was no effect after taking mexiletine. In addition, the variant did not cause the same shift when cells were treated with lidocaine, a structurally similar drug also used to treat arrhythmia, which they say suggests something specific about how mexiletine interacts with S1103Y channels.
Interestingly, the effect of mexiletine on the gene variant was only apparent in the cells derived from the human and entirely absent in the genetically matched cell line.
"This is exactly why the field is moving toward more physiologically relevant models," Silva said. "If we had stopped at the expression system, we would have missed the most clinically important finding entirely."
The work aligns with the National Institute of Health's push toward New Approach Methodologies, a framework that prioritizes human-relevant, cell-based models over traditional approaches that may not capture the complexity of human biology.
"We're demonstrating a fundamental concept in precision medicine," Silva said. "Preserved channel function doesn't guarantee a preserved pharmacological response. A variant that looks benign in isolation can have real consequences when you introduce a drug."
Co-investigators include Nathaniel Huebsch, associate professor of biomedical engineering in McKelvey Engineering; Jonathan D. Moreno, MD, PhD, assistant professor, and Jennifer NA Silva, MD, the James G. Berges and Elizabeth Mannen Berges Professor of Pediatric Cardiology, both at WashU Medicine.
The team says it hopes the findings will motivate clinical studies to determine whether genetic testing for S1103Y, and potentially other common ion channel variants, should inform prescribing decisions for patients who might benefit from antiarrhythmic drug therapy.
Marras M, Josef JD, Schuster T, Struckman HL, Wagner ES, Lee L, Smith KJ, Amsler JM, Woodbury LS, Marquez E, Huebsch N, Moreno JD, Silva J NA, Silva, JR. Common Genetic Variants of the Cardiac Sodium Channel Alter Patient Response to Class 1b Antiarrhythmics. Journal of Precision Medicine, published online March 18, 2016. DOI: 10.1016/j.premed.2026.100034
Funding for this research was provided by the National Heart, Lung, and Blood Institute of the National Institutes of Health (R01 HL148803) and the American Heart Association (24PRE1198562, 960621).